Dr. Langenhan is from the Perelman School of Medicine, University of Pennsylvania, Philadelphia. Dr. Novoa is from the Departments of Pathology and Dermatology, Stanford Medical Center, California. Dr. Pappas-Taffer is from the Department of Dermatology, Perelman Center for Advanced Medicine, University of Pennsylvania.
The authors report no conflicts of interest.
Correspondence: Lisa Pappas-Taffer, MD, Department of Dermatology, University of Pennsylvania, Perelman Center for Advanced Medicine, 3400 Civic Center Blvd, Philadelphia, PA 19104 (lisa.pappas-taffer@uphs.upenn.edu).
Port-wine stains (PWSs), or capillary malformations, are common congenital lesions, but acquired lesions rarely present in the setting of trauma. We present the case of an 18-year-old man who developed a PWS and associated localized eczema following penetrating trauma to the left abdomen. The diagnoses were confirmed on biopsy. The patient’s eczema improved with topical steroids. Magnetic resonance imaging of PWSs is recommended in order to rule out deeper arteriovenous malformations. More research is needed to elucidate the connection between PWS pathophysiology and the development of eczema.
Port-wine stains (PWSs) most often are congenital lesions but can present later in life as acquired lesions with the same clinical and histologic findings.
Magnetic resonance imaging of acquired PWSs should be considered to rule out underlying vascular anomalies (eg, deeper arteriovenous malformations).
Pulsed dye laser therapy is safe for darker skin types and is the treatment of choice for acquired PWSs.
References
Port-wine stains (PWSs) are common congenital capillary vascular malformations with an incidence of 3 per 1000 neonates.1 Rarely, acquired PWSs are seen, sometimes appearing following trauma.2-5 Port-wine stains are diagnosed clinically and present as painless, partially or entirely blanchable pink patches that respect the median (midline) plane.6 Although histopathologic examination is not necessary for diagnosis of PWS, typical findings include dilated, ectatic capillaries.7,8 Since it was first reported by Traub9 in 1939, more than 60 cases of acquired PWSs have been reported.10 A PubMed search of articles indexed for MEDLINE using the search terms acquired port-wine stain and port-wine stain and eczema yielded no cases of acquired PWS with associated eczematous changes and only 30 casesof congenital PWS with superimposed eczema.11-18 We report the case of an acquired PWS with superimposed eczema in an 18-year-old man following penetrating abdominal trauma.
Case Report
An otherwise healthy 18-year-old man presented to our dermatology office for evaluation of an eruption that had developed at the site of an abdominal stab wound he sustained 2 to 3 years prior. One year after he was stabbed, the patient developed a nonpruritic, painless red patch located 1 cm anterior to the healed wound on the left abdomen. The patch gradually grew larger to involve the entire left abdomen, extending to the left lower back. The site of the healed stab wound also became raised and pruritic, and the patient noted another pruritic plaque that formed within the larger patch. The patient reported no other skin conditions prior to the current eruption. His medical history was notable for seasonal allergies and asthma, but no childhood eczema.
Physical examination revealed a healthy, well-nourished man with Fitzpatrick skin type IV. A red, purpuric, coalescent patch with slightly arcuate borders extending from the mid abdomen to the left posterior flank was noted. The left lateral aspect of the patch blanched with pressure and respected the median plane. Within the larger patch, a 4-cm×2-cm lichenified, slightly macerated, hyperpigmented plaque was noted at the site of the stab wound (Figure 1). Based on these clinical findings, a presumptive diagnosis of an acquired PWS with superimposed eczema was made.
Figure 1. A lichenified, macerated, hyperpigmented plaque on the left lower abdomen with a larger red, coalescent patch with slightly arcuate borders that respected the median plane.
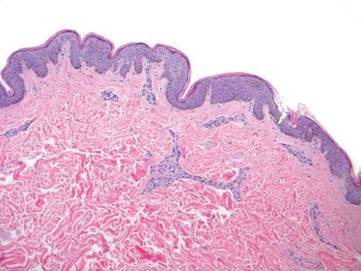
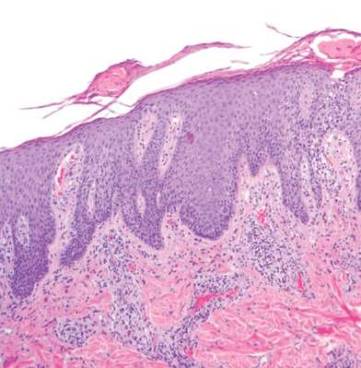
Punch biopsy specimens were taken from the large vascular patch and the smaller lichenified plaque. Histopathologic examination of the vascular patch showed an increased number of small vessels in the superficial dermis with thickened vessel walls, ectatic lumens, and no vasculopathy, consistent with a vascular malformation or a reactive vascular proliferation (Figure 2). On histopathology, the plaque showed epidermal spongiosis and hyperplasia with serum crust and a papillary dermis containing a mixed inflammatory infiltrate with occasional eosinophils, consistent with an eczematous dermatitis (Figure 3). The histologic findings confirmed the clinical diagnosis.
Figure 2. A biopsy specimen from the large patch on the left flank showed an increased number of small vessels and thickened vessel walls consistent with vascular malformation (H&E, original magnification ×100).
Figure 3. A biopsy specimen from the hyperpigmented plaque showed serum crust, hyperplasia, spongiosis, and a mixed inflammatory infiltrate with occasional eosinophils in the papillary dermis consistent with eczematous dermatitis (H&E, original magnification ×100).
The pruritic, lichenified plaque improved with application of triamcinolone ointment 0.1% twice daily for 2 weeks. Magnetic resonance imaging to rule out an underlying arteriovenous malformation was recommended, but the patient declined.